
38 yo female presents with altered mental status. The patient was found down at home, and no further history is known. EMS intubated on scene. On arrival, pt’s vitals are as follows: HR 136, BP 97/54, RR 18 (artificial), T 102.3F, O2 sat 96% on 100% FiO2.

Answer: Infectious endocarditis
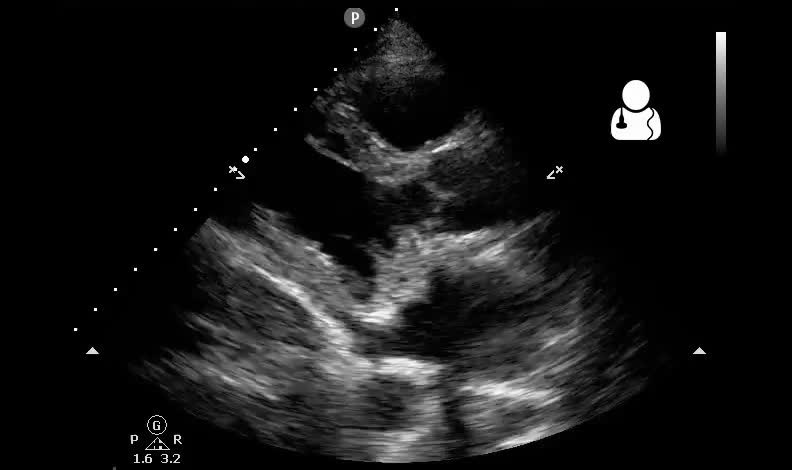
The patient in question had an artificial valve due to previous intravenous drug use. Bedside echocardiography showed valve stenosis as well as vegetations on the mitral valve, and likely on the tricuspid valve. IV antibiotics were started immediately and the patient was stabilized. Unfortunately, the patient died 3 days later due to complications of her endocarditis.
- Endocarditis is a disease that carries significant morbidity and mortality.1
- The initial presenting symptoms can be nonspecific and mimic many other diseases,2 but
 early diagnosis is crucial as this disease has been reported to have an in-hospital mortality rate as high as 18%,2 and an overall mortality rate within one year of around 33% for all comers.1
early diagnosis is crucial as this disease has been reported to have an in-hospital mortality rate as high as 18%,2 and an overall mortality rate within one year of around 33% for all comers.1 - Although TEE is considered the gold standard for an imaging diagnosis, TTE can be a viable alternative. With TEE as the reference criterion, Erbel et al found that 70% of valvular vegetations between 6-10mm were identified by TTE.3
- Having a high sensitivity for detecting larger lesions is crucial as the size of the vegetation was found to be the only important predictor of in-house mortality.4
- Many patients with endocarditis will develop some degree of regurgitation due to failure of the valve at the closure line or a perforation in the leaflet itself. A few will develop mitral stenosis as we see here.5
- Mitral stenosis may be more common in those with a history of prosthetic valves because of the propensity for the infection to involve the area around the ring of the valve rather than the leaflets.5
Jacob Avila, MD, RDMS
- Thuny F, Grisoli D, Collart F, Habib G, Raoult D. Management of infective endocarditis: challenges and perspectives. Lancet. 2012;379(9819):965-75.
- Seif D, Meeks A, Mailhot T, Perera P. Emergency department diagnosis of infective endocarditis using bedside emergency ultrasound. Crit Ultrasound J. 2013;5(1):1.
- Erbel R, Rohmann S, Drexler M, Mohr-Kahaly S, Gerharz CD, Iversen S, Oelert H, Meyer J (1988) Improved diagnostic value of echocardiography in patients with infective endocarditis by transesophageal approach. A prospective study. Eur Heart J 9(1):43–53
- Nunes MCP, Gelape CL, Ferrari TCA (2010) Profile of infective endocarditis at a tertiary care center in Brazil during a seven year period: prognostic factors and in-hospital outcome. Int J Infect Dis 14:e394–e398
- Otto, Catherine M. Textbook of clinical echocardiography. 5th ed. Philadelphia, PA: Elsevier/Saunders, 2013. Print. p 247
